TOTAL HIP REPLACEMENT
If the hip is severely damaged by arthritis, fracture or any other condition, it will be hard for the patient to perform simple activities such as, walking, climbing stairs, bending or sitting. If the hip is stiff, it may be hard to put on the shoes and socks. If nonsurgical treatments like medications are no longer helpful, that means the patient needs total hip replacement surgery. Joint replacement surgery helps the patients to relieve pain and to do daily activities.
Common Causes of Hip Pain
The most common cause of chronic hip pain and disability is arthritis. Although there are many types of arthritis, most hip pain is caused by just five types: osteoarthritis, rheumatoid arthritis, post-traumatic arthritis, osteonecrosis and childhood hip disease.
1)Osteoarthritis
Osteoarthritis is the most common form of arthritis in the hip. It is a degenerative, wear-and-tear type of arthritis that occurs most often in people 50 years of age and older. In osteoarthritis, the cartilage in the hip joint gradually wears away. As the cartilage wears away, it becomes frayed and rough, and the protective space between the bones decrease. This can result in bone rubbing on bone, and produce painful bone spurs. Osteoarthritis develops slowly and the pain it causes worsens over time.
2)Rheumatoid Arthritis
Rheumatoid arthritis is a chronic autoimmune disease (immune system attacks its own tissues) that attacks multiple joints throughout the body. The immune system damages normal tissue (such as cartilage and ligaments) and softens the cartilage. This chronic inflammation damages the cartilage and eventually cause cartilage loss, pain, and stiffness.
3)Posttraumatic Arthritis
Posttraumatic arthritis develops after a serious hip injury. For example, acetabulum fracture, the fracture and dislocation of femur head may damage the joint surface and lead to arthritis years after the injury.
4)Osteonecrosis
The lack of blood may cause the surface of the bone to collapse, and arthritis will result. This is called osteonecrosis (also sometimes referred to as avascular necrosis). Some diseases such as sickle cell anemia and Gaucher's disease and long- term use of alcohol and cortisone can cause osteonecrosis.
5)Childhood hip disease
Some childhood hip pathologies such as hip dysplasia, Perthes disease, slipped capital femoral epiphysis (SCFE), and enfection cause osteoartritis later on in life.
What is a hip replacement and how is it done?
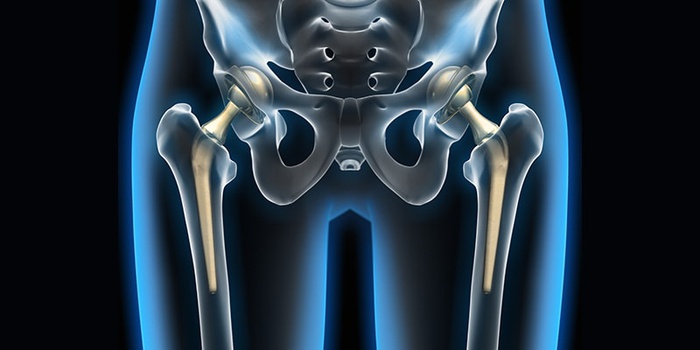
In a total hip replacement (also called total hip arthroplasty), the damaged bone and cartilage is removed and replaced with prosthetic components. The damaged femoral head is removed and replaced with a metal stem that is placed into the hollow center of the femur with cemented or press fit. A metal or ceramic ball is placed on the upper part of the stem.The damaged cartilage surface of the socket (acetabulum) is removed and replaced with a metal socket. Screws are used to hold the socket in place.A plastic, ceramic, spacer is inserted between the new ball and the socket to allow for a smooth gliding surface.
When Surgery Is Recommended
People who benefit from total knee replacement are as follows:
*When the patient has severe knee pain or stiffness that limits daily activities, such as walking, climbing stairs and if it is hard to put on the shoes and the socks. *When the pain does not improve with other treatments such as anti-inflammatory medications, cortisone injections, lubricating injections and physical therapy.
There are no absolute age or weight restrictions for total hip replacement surgery. Recommendations for surgery are based on a patient's pain and disability.
Orthopaedic Evaluation
The orthopedics surgeon does the phyisical examination of the patient, gets his/her medical history and needs some imagings (X-Ray, MRI) and laboratory tests to decide about the treatment and plan about the operation. In addition, the orthopaedic surgeon will explain the potential risks and complications of total hip replacement, including those related to the surgery itself and those that can occur over time after the surgery.
Recovery
The success of the surgery will depend in large measure on how well the patient follow the orthopaedic surgeon's instructions regarding home care during the first few weeks after surgery.
Activity
Exercise is a critical component of home care, particularly during the first few weeks after surgery. The patient should be able to resume most normal light activities of daily living within 3 to 6 weeks following surgery. The activity program should include:
*A graduated activity program to slowly increase the mobility, such as sitting, standing, and climbing stairs initially in the home and later outside *Specific exercises several times a day to restore movement and strengthen the hip.
Possible Complications of Surgery
The complication rate following total hip replacement is low. Serious complications, such as a hip joint infection, blood clots, implant problems, continued pain and neurovascular injury are less than 2%.
Infection: Infection may occur in the wound or deep around the prosthesis. Minor infections in the wound area are generally treated with antibiotics. Major or deep infections may require more surgery and removal of the prosthesis.
Blood clots: Blood clots in the leg veins are a common complication of knee replacement surgery. Blood clots can form in the deep veins of the legs or pelvis after surgery. To prevent blood clot the patient should do periodic elevation of the legs, lower leg exercises to increase circulation, support stockings, and blood thinners such as warfarin (Coumadin), low-molecular-weight heparin, and aspirin can help prevent this problem.
Implant problems: Although implant designs and materials continue to advance, implant surfaces may wear down and the components may loosen.
Continued pain: A small number of patients continue to have pain after a hip replacement. This complication is rare.
Neurovascular injury: While rare, injury to the nerves or blood vessels around the hip can occur during surgery.
Leg-length Inequality: The orthopaedic surgeon will make every effort to make the patient leg lengths equal. Sometimes after a hip replacement, one leg may feel longer or shorter than the other.
Dislocation: This occurs when the ball comes out of the socket and it is uncommon. The risk for dislocation is greatest in the first few months after surgery while the tissues are healing. If the ball does come out of the socket, a closed reduction usually can put it back into place without the need for more surgery. In situations in which the hip continues to dislocate, further surgery may be necessary.
Loosening and Implant Wear: Over years, the hip prosthesis may wear out or loosen. This is most often due to everyday activity. It can also result from a biologic thinning of the bone called osteolysis. If loosening is painful, a second surgery called a revision may be necessary.
© COPYRIGHT 2025 ALL RIGHTS RESERVED
Privacy Policy